
 ENOUS INSUFFICIENCY IS the underlying problem that leads to varicose veins and much more. It occurs when faulty valves allow the blood in the veins to flow backwards and pool in the lower half of the body. The increased pressure from the pooled blood leads to additional veins becoming elongated, dilated and gnarled (or varicose). In turn, these veins fail, leading to greater compromise of proper blood flow back to the heart. Under the force of gravity, the increasing pool of uncirculating venous blood leads to venous hypertension. Venous hypertension leads to inflammation and congestion in the tissue of the legs and is responsible for the symptoms of venous insufficiency, which can include edema, pain, aching skin discoloration, leg cramping, leg fatigue and restlessness.
ENOUS INSUFFICIENCY IS the underlying problem that leads to varicose veins and much more. It occurs when faulty valves allow the blood in the veins to flow backwards and pool in the lower half of the body. The increased pressure from the pooled blood leads to additional veins becoming elongated, dilated and gnarled (or varicose). In turn, these veins fail, leading to greater compromise of proper blood flow back to the heart. Under the force of gravity, the increasing pool of uncirculating venous blood leads to venous hypertension. Venous hypertension leads to inflammation and congestion in the tissue of the legs and is responsible for the symptoms of venous insufficiency, which can include edema, pain, aching skin discoloration, leg cramping, leg fatigue and restlessness.
“Untreated venous issues can lead to a multitude of serious health problems, including variceal bleeding, venous ulcers and blood clots, also known as deep venous thrombosis,” says Thomas Wright, M.D., FACP, RVT, Medical Director of Laser Lipo & Vein Center in St. Louis, MO. “It’s important to dispel the myth that venous insufficiency is just a cosmetic issue. Leaving venous issues untreated can eventually lead to much larger problems.”
Venous insufficiency can be the underlying cause for a plethora of other conditions, including lower extremity cellulitis, restless legs syndrome and leg cramps. According to Dr. Wright, when patients present with venous insufficiency symptoms, physicians often only check some of the obvious explanations and do not delve deeper to look for the possibility of venous reflux as an underlying cause.
For example, patients with venous insufficiency may experience leg cramps. When patients report this symptom, physicians often check potassium and calcium levels, but they seldom refer patients for a venous Doppler exam, even in patients’ symptoms are worse after standing of if they have physical signs of venous insufficiency, such as spider veins or skin changes. “There’s a large percentage of people walking around with venous problems who aren’t
Venous Insufficiency, Venous Stasis Dermatitis and Cellulitis
Patients with venous insufficiency often develop a rash on the legs called stasis dermatitis.

The increased venous pressure in the legs is transmitted to the capillaries. The pressure leads to the release of red blood cells and other inflammatory substances that produce a reddish discoloration of the skin. This rash responds best to lubrication or a mild steroid cream and compression stockings or wraps to counterbalance the venous hypertension. Ultimately, the best treatment is the correction of the underlying cause of venous insufficiency.
Additionally, because of the underlying inflammation in the skin, patients with venous insufficiency are also prone to developing cellulitis. Cellulitis is a potentially serious bacterial skin infection – most commonly occurring in the skin on the lower legs – that can affect both the skin’s surface and its underlying tissue. It is often difficult to know for sure whether the reddened, tender and swollen leg is caused by venous insufficiency alone or if there is a bacterial infection as well. Antibiotics should be used to treat the cellulitis; however, if the underlying cause is venous insufficiency, cellulitis will likely return if the root cause is not treated.
Venous Insufficiency and Lower-Extremity Edema
Venous hypertension is the most common cause of tissue edema in the lower extremity, and the most common cause of venous hypertension is venous reflux. Congestive heart failure is a distant second. The edema in the legs caused by venous insufficiency is often worse in one leg and often involves less fluid accumulation than the edema caused by heart failure. However, venous hypertension also affects the lymphatic drainage and can lead to massive lower-leg edema (veno-lymphedema). Despite the significantly greater prevalence of primary venous insufficiency,
MEET THE DOCTOR
THOMAS WRIGHT, M.D., FACP, Medical Director of Laser Lipo & Vein Center in St. Louis, MO, was one of the first 200-plus surgeons in the nation to become board certified in phlebology by the American Board of Phlebology. Dr. Wright attended Duke University for his undergraduate degree and earned his medical degree from the University of Missouri in Columbia, MO. Dr. Wright completed his residency at the University of Alabama at Birmingham.
His professional affiliations include the American College of Phlebology, the American Medical Association, the American Society of Laser Medicine and Surgery, the Missouri State Medical Association, the American Academy of Cosmetic Surgery and the American Registry for Diagnostic Medical Sonography.
Dr. Wright has authored and presented several scientific papers on surgical techniques in the treatment of venous insufficiency.
it is often not considered even after cardiac, heptic and renal problems have been ruled out as the cause of the edema.
Venous Insufficiency and Restless Legs Syndrome
Restless legs syndrome is believed to be associated with a number of factors, including iron deficiency, peripheral neuropathy, Parkinson’s disease and other neurological disorders. Recent medical research reported in the journal Dermatologic Surgery, showed that 22% of patients with restless legs syndrome also have venous insufficiency as revealed through Doppler examination. “Symptoms of restless legs syndrome include burning and tingling sensations and the uncontrollable urge to move the legs,

NOT JUST A COSMETIC CONCERN
VENOUS INSUFFICIENCY AND the associated varicose veins are not just a cosmetic concern; they can result in physical symptoms. Signs of venous insufficiency include: varicose veins; leg swelling; skin changes, such as redness or a brownish staining and a whitish loss of skin pigment; and ulcers on the legs. Symptoms of venous insufficiency include: leg and pelvic pain or cramping; a feeling of throbbing, aching or heaviness in th elegs; leg fatigue; and restlessness.
Most insurance companies cover symptomatic venous disease, meaning patients don’t have to live with the discomfort associated with venous disorders. Laser Lipo & Vein Center in St. Louis accepts all major insurance coverage.
To refer a patient to Laser Lipo & Vein Center, call (636) 397-4012.
which is worse at night when laying down and is relieved by movement or walking,” says Dr. Wright. “There is a great overlap in the sumptoms of vein disease and restless legs syndrome. As the two conditions have similar presentations, it’s important to consider both the vascular and neurological concerns.”
Studies show that the treatment of venous insufficiency can relieve symptoms of restless leg syndrome. According to a study in the journal Phlebology, in patients with restless leg syndrome and venous insufficiency, 98% of patients experienced relief from restless legs syndrome symptoms by treating their venous insufficiency, and 80% had long-term relief.
Before comitting a patient with restless legs syndrome to possible life-long medication with potential side effects, venous insufficiency should be checked as a possible cause, as correction of the vein reflux provides long-term and likely permanent relief.
Making a Diagnosis
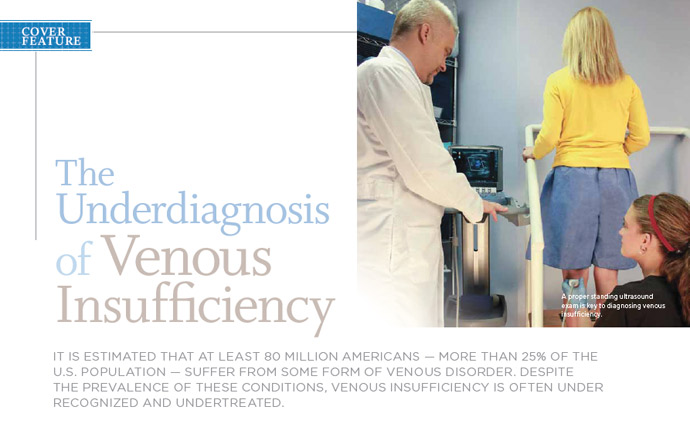
Correctly diagnosing vein disease involves a review of the patient’s history of symptoms, physical examination and a duplex ultrasound of the veins. The duplex ultrasound exam can help identify the presence of reflux and its location, as well as determine the patency of the deep and superficial venous systems. The leg is examined from the saphenofemoral junction down to the ankle.
The key to a successful ultrasound is that the patient is standing during the exam to accurately determine blood flow concerns. Venous insufficiency can be easily missed in the event that the ultrasound is performed while the patient is lying down.
“Often, when you send a patient for an ultrasound evaluation for venous disease, the technician mistakenly has the patient lie down. This occurs because many technicians are trained to look for deep vein disease; however, this positioning will result in an inadequate exam, and superficial venous insufficiency won’t be diagnosed,” says Dr. Wright. “It’s Important to send patients to a specialized vein venter, as their sonographers are trained to detect venous insufficiency and can diagnose it with more accuracy.”
Once venous insufficiency has been correctly identified, a variety of conservative treatment methods may be utilized as an initial treatment approach. These may include elevating the



AN UP-AND-COMING SPECIALTY
PHLEBOLOGY IS A relatively new medical specialty that focuses on the study and treatment of venous diseases and disorders. As more than 80 million Americans currently suffer from venous disorders, phlebology now offers the opportunity for patients to see a dedicated specialist who is up to date on the latest diagnostic techniques and treatment methods. Phlebologists address a variety of venous concerns, including varicose veins, spider veins, deep vein thrombosis, pulmonary embolism and venous insufficiency.
A BRIEF HISTORY
The American College of Phlebology was first founded in 1986 – then named the North American Society of Phlebology – and has grown during the last 20 years to begin to fulfill its mission of advancing vein care and supporting new clinical research in the field of venous disease. This research has resulted in new pharmacological advances and minimally invasive surgical techniques for the treatment of venous disorders.
After 20 years of dedicated work, the American College of Phlebology succeeded in its goal of offically establishing phlebology in the medical community – the American Medical Association recognized phlebology as its own self-designated medical specialty in 2005.
The first American College of Phlebology fellowship program began offering 12 months of phlebology postgraduate training in 2007, and physicians were first given the opportunity to take the American Board of Phlebology certification exam in May of 2008. The American College of Phlebology is now working to establish a registry-level phlebology ultrasound examination for ultrasound specialists.
The American College of Phlebology publishes its own official journal, Phlebology.
legs when possible, avoiding long periods of sitting or standing, wearing compression stockings and being active. if these methods are not successful, a variety of surgical or procedural options may be recommended.
Treatment in the Laser Era
Vein stripping or vein ligitation of the saphenous vein was once the primary method for treatment of varicose veins and its underlying cause. It involves tying off and stripping out the damaged vein. Vein stripping usually requires a recovery period of six weeks or more and can involve significant postoperative pain.
Today, endovenous laser ablation (ELA) offers a minimally invasive alternative to the surgical stripping of veins.
“ELA has an impressive 98% successful long-term saphenous closure and very low recurrence rate,” says Dr. Wright. “This compares favorably with vein stripping, which has a recurrence rate of up to 40%.”
The nonsurgical procedure inserts a small probe with a

laser fiber through a freckle-sized nick in the skin. Ultrasound guidance helps direct the probe to the damaged vein. Pulses of laser light are delivered into the vein, causing the internal vein wall to collapse and seal shut. This 45-minute, minimally invasive treatment can be performed in a single office visit with local anesthesia.
“Unlike vein stripping, there is no scarring or long recovery period with ELA. The procedure is about as invasive as having a peripheral IV,” says Dr. Wright. “Patients are up and walking the same day and can resume normal activities within a day or two.”
Other treatment options for venous disorders include:
+ Sclerotherapy is a treatment that uses a tiny needle to inject a solution called sclerosant into the veins. This solution irritates the lining of the veins and causes them to close. The body then absorbs the treated vein. Sclerotherapy can be used to treat both varicose and spider veins that are often seen on the surface of the legs. For Deeper branches of vein that may not be seen on the surface, an ultrasound-guided option is also available. Multiple treatments are usually required to permanently close a vein.
+ Veinwave is a new device approved by the U.S. Food and Drug Administration just this year. It has been used in Europe for more than eight years. While sclerotherapy is successful in the treatment of most large and small veins, it cannot treat the fine, reddish veins on the knees, ankles and face. The new Veinwave device sends radiowave energy in quick pulses to the affected area, causing the vein walls to collapse. Unlike
similar devices available before, Veinwave is virtually painless and has no risk of burning the skin.
“This device was developed as a way to treat the tiny veins on the surface of the skin that cannot be treated with sclerotherapy,” says Dr. wright. “The other options of treating these tiny veins – laser and light treatments – pose the risk of burning and scarring.
“ELA remains the quickest, most effective procedure for venous insufficiency, and it’s changing the face of treatment,” says Dr. Wright. “ELA has lowered the bar for patients, because it is so much less invasive and promotes a rapid recovery, making treatment for venous insufficiency a possibility for a greater range of people. Now, patients don’t have to wait until they are miserable from the symptoms or have developed complications to be treated.”
Referring Your Patients
For patients living with the pain and discomfort associated with venous insufficiency, help is available. Laser Lipo & Vein Center in St. Louis offers comprehensive care for venous disease, from diagnosis to treatment.
For more information, visit lasermenu.wpengine.com. To refer a patient, call (636) 397-4012.
![]()
Reprinted from St. Louis BI-State MD NEWS STLOUIS.MDNEWS.COM