Although lipedema was first described by Dr. Edgar Allen and Dr. Edgar Hines in 1940 at the Mayo Clinic, many physicians remain unaware of this medical condition or its symptoms.
What is Lipedema?
Lipedema is a chronic progressive medical disease that causes disproportionate swollen fat deposition in the arms and legs. Lipedema is disproportionate, meaning that fat accumulation is much more significant in the legs and/or arms than in the rest of the body. As lipedema worsens, it causes symptoms in the limbs, which feel heavy and can be painful. Lipedema is associated with easy bruising, especially in the affected limbs. As a result of the lack of awareness, many patients are not diagnosed or properly treated or not treated until they have progressed to more advanced stages of the disease.
Other Names and Synonyms of Lipedema
Lipedema is also called lipoedema or lipodema, the “swollen fat syndrome”, and the “painful fat syndrome.” In medical literature, lipedema is also referred to by the following medical terms: Lipohyperplasia Dolorosa, Lipalgia, Adipoalgesia, Adiposis Dolorosa, Lipomatosis Dolorosa of the legs, and Lipohypertrophy Dolorosa.
What Can Be Confused With Lipedema?
Lipedema is well known in Germany and the Netherlands; many textbooks and articles are written about the condition. Although it was initially described here in the United States, lipedema is not well known, and articles and texts are few. This results in confusion and a lack of recognition. Obesity, which causes increased fat all over the body, including the stomach, is sometimes confused with Lipedema. Lipohypertrophy or cellulite, which also causes a disproportionate fat accumulation in the legs, but does not cause pain or swelling, is often confused with lipedema. Lymphedema is also often confused with lipedema. Lymphedema is asymmetric swelling of the limbs often only one arm or leg is affected. Lymphedema causes swelling down to the feet and hands, whereas lipedema spares the hands and feet. Lymphedema is not painful or associated with easy bruising like lipedema. Chronic venous insufficiency can cause swelling and pain; however, it is not usually symmetric, has associated and characteristic skin changes, and usually has varicose veins.
Causes of Lipedema and Pathogenesis
The exact cause and parthenogenesis of lipedema are not known. It is considered a genetic disorder with autosomal dominant inheritance and sex limitation [2]. It occurs much more frequently in first and second-degree relatives of affected individuals. Reported rates of family clustering are from 16% to 64% of cases [3] [4]. Lipedema usually occurs in women, although it can occur in men. Hormonal influences play a role in the development and progression of the disease, and in the majority of patients, the disease usually starts imperceptibly after puberty. Still, it may also develop at other periods of hormonal change, such as pregnancy or menopause.
Stages of Lipedema
As patients work through getting an official lipedema diagnosis, experts will first need to determine what lipedema stage the patient is currently at. There are three different lipedema stages, or levels of progression, used to evaluate how far the disease has progressed in the affected areas of the body – the first stage is the earliest onset, and the third stage is the most progressed.
The Three Stages of Lipedema:
- Stage 1 Lipedema: skin is somewhat enlarged but smooth. Small nodules may be felt under the surface of the skin.
- Stage 2 Lipedema: The skin looks bumpy on the surface.
- Stage 3 Lipedema: increased fat hypertrophy and larger subcutaneous nodules.

As lipedema progresses through these three stages, pain, tenderness, swelling, and fat accumulation may increase. The images below provide an overview of the three lipedema stages, showing the location of fat build-up plus the resulting body shape at each stage. Depending on the person, different body parts can be affected in different ways at each stage.
Types of Lipedema

The Types of lipedema describe the body areas where the lipedema disease is present. More simply, these types refer to the location of the lipedema fat. The 5 types of lipedema were first described by Scmeller and Meier Vollrath, and the criteria by Meier-Volarath in 2007, as described below.
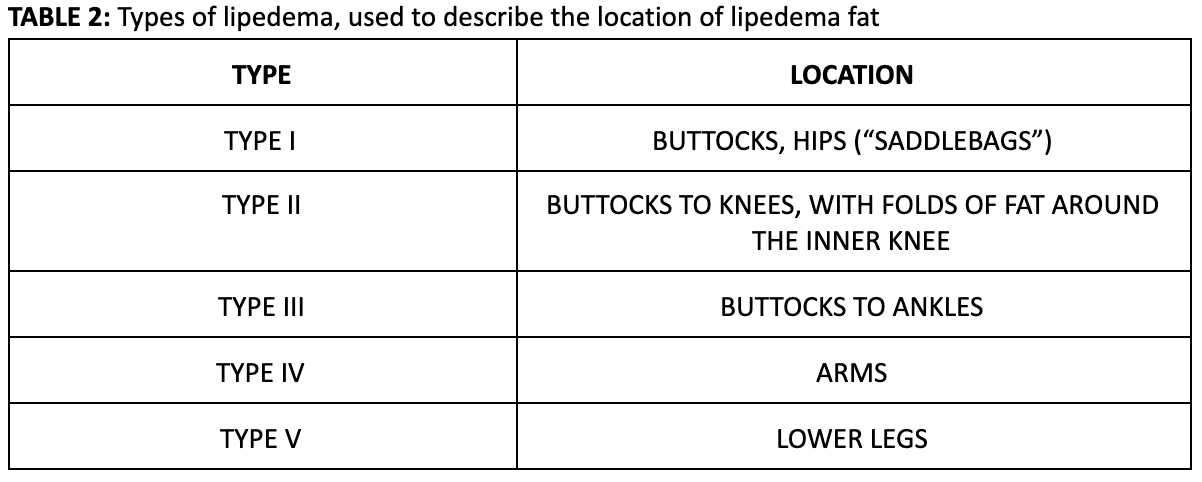
Lipedema Type 1: Buttocks, Hips (“Saddlebags”)

Lipedema Type 2: Upper Legs

Lipedema Type 3: Entire Lower Body

Lipedema Type 4: Arms

Lipedema Type 5: Lower Legs
Getting a Lipedema Diagnosis
No specific blood or imaging test is widely available to diagnose lipedema. Lipedema’s diagnosis is based on a clinical evaluation using the below criteria by a physician knowledgeable and experienced in diagnosing the disease and with supporting tests that rule out other diagnoses. Lipedema is a poorly recognized and under-appreciated disease in the United States. It is estimated that 11% of the female population has this condition. However, the diagnosis is rarely made by US physicians, which is largely a result of poor awareness and understanding. Recognizing the characteristic features of Lipedema’s early stages and eliminating other conditions that can be confused with lipedema is the key to the proper diagnosis of lipedema.
Lipedema’s diagnosis is based on a clinical evaluation from a physician with specific knowledge and experience of the disease and with supporting tests that rule out other diagnoses. Lipedema is a poorly recognized and under-appreciated disease in the United States. It is estimated that 11% of the female population has this condition. However, US physicians rarely make the diagnosis, mainly due to poor awareness and understanding. The recognition of characteristic features of Lipedema’s early stages and the elimination of other conditions that can be confused with lipedema. Continue reading to learn more about lipedema’s early stages and its signs!
International Consensus for Diagnosing Lipedema:
- Uncontrolled localized deposition of fat in the lower extremities
- Symmetric increase in adipose tissue (two-body syndrome)
- Onset at puberty, pregnancy, and menopause
- Women (usually progressive with age)
- Easy Bruising
- Tired or heavy legs
- Mild or severe pain or pressure to touch
- Hands and feet are usually spared
- Cuffing or bulging at the joints
- Stemmer’s sign is negative
- Nodules of fat are palpable
- Limited mobility and decreased social activity*
*Adapted from Sandhofer M, et al. Dermatol Surg 2020;46(2):220-228.
Resources for Lipedema
» Common Myths about Lipedema
» Compression Stockings for Lipedema
» Liposuction for Lipedema
» Lipedema Seminar Overview
» Lymph Sparing Liposuction
» Manual Lymphatic Drainage
» Natural Treatment for Lipedema
» Where Does Lipedema Fat Accumulate?
Treatment
Conservative therapy with combined decongestive therapy (CDT) has a long track record as being an effective lipedema treatment. The central component of CDT is Manual Lymphatic Drainage (MLD), which is light massage therapy started centrally with a pump and scoop motion toward the heart. The manual lymph drainage is combined with compression wraps to complete the CDT. This conservative therapy can reduce circumference by approximately 10% and improve pain and symptoms of hypersensitivity to pressure. If the CDT is discontinued, the swelling and symptoms return. Compression stockings, which often need to be custom fit, can help maintain the progress of combined decongestive therapy. However, the compression only works for the swelling component of the lipedema and does not address the lipo-hypertrophy or excess fat.
Surgical treatment has become much more common in the last fifteen years and offers a greater chance of sustained improvement. Liposuction surgery of old was performed with general anesthesia, not tumescent anesthesia, and was associated with postsurgical complications and lymphatic vessel damage and was not an effective lipedema treatment. However, modern tumescent liposuction performed with a wet tumescent technique is not associated with significant bleeding and does not damage superficial lymphatic vessels according to macroscopic and anatomical studies[6][7]. The application of blunt micro cannulas measuring 2mm – 4mm allows surgeons to use a gentler technique and avoid damaging important structures, which results in a faster recovery and a significant net improvement of lipedema symptoms. Dr. Wright has modified the liposuction technique developed by Dr. Jeffery Klein and Dr. Stefan Rapprich[8] to include preoperative assessment and mapping of lymphatics to minimize the chance of lymphatics injury. The tumescent liposuction procedure not only improves physical appearance by returning some balance to the body’s proportion, it also can significantly reduce and eliminate the symptoms. Postoperatively combined decongestive therapy should be initiated or continued with strict compression adherence.



Long-term studies show that true tumescent lipedema liposuction can improve fat reduction if appropriately performed by surgeons. It can reduce the circumference of the hips and lower extremities, balancing the disproportionality of the upper and lower parts of the body, and can improve or contribute to the relief of pain and pressure sensitivity, even reduce disability over an extended period. However, the tendency for edema usually persists, and physical therapy and compression is often still necessary for patients, but to a lesser degree.
In conclusion, tumescent lipedema liposuction surgery is a great lipedema treatment and provides significant improvement in body shape, improvement of symptoms, and improvement in mobility. It also lessens the need for conservative treatment and significantly increases quality of life. Because of the level of expertise and understanding required to successfully perform tumescent liposuction surgery on these patients, they should seek treatment in centers where the surgeon and staff are specifically trained in lymphology and the needs of these unique patients. Call today for more information about our liposuction for lipedema treatment. For even more information, you may want to read here.
[1] Allen E. Hines, Lipedema of the legs: A Syndrome Characterized by Fat Legs and Orthostatic Edema. (Proc Staff Meet Mayo Clinic), 1940; 15184-187.
[2] A.H. Child, K.D. Gordon, P. Scharpe et al. Lipedema: An Inherited Condition. (Am J Med Genet A 2010), 152:970-6. PMID: 20358611 (PubMed – Indexed for MEDLINE).
[3] L.E. Wold, E.A. Hines, E.V. Hines, Lipedema of the Legs: A Syndrome Characterized by Fat Legs and Edema. (Ann Intern Med) 1949; 34: 1243-1250.
[4] C.A. Harwood, R.H. Bull, J. Evans, P.S. Mortimer, Lymphatic and Venous Function in Lipedema. (Br J Dermatol) 1996; 134: 1-6.
[5] Herpertz U. Krankheitsspektrum, des Lipödems an einer Lymphologischen, Fachklinik – Erscheinungsformen, Mischbilder und Behandlungsmöglichkeiten, vasomed 1997; 5: 301-307.
[6] A. Frick, J.N. Hoffmann, R.G.H. Baumeister, R. Putz, Liposuction Technique and Lymphatic Lesions in Lower Legs: Anatomic Study to Reduce Risks, (Plast Reconstr Surg) 1999; 103: 1868-1873.
[7] J.N. Hoffmann, J.P. Fertmann, R.G. Baumeister, R. Putz, A. Frick, Tumescent and Dry Liposuction of Lower Extremities: Differences in Lymph Vessel Injury, (Plast Reconstr Sur) 2004; 113: 718-724; discussion 725-726.
[8] S. Rapprich, A. Dingler, M. Podda, Liposuction is an Effective Treatment for Lipedema Results of a Study with 25 Patients, Department of Dermatology, Darmstadt Hospital, Germany, (JDDG Journal of the German Society of Dermatology) 20011; 9.33-40 DOI: 10.1111/j.1610-0387.2010.07504.x